DEA Narcotic Tracking Requirements for EMS: What Your Agency Needs to Know
Why DEA Oversight Matters for EMS
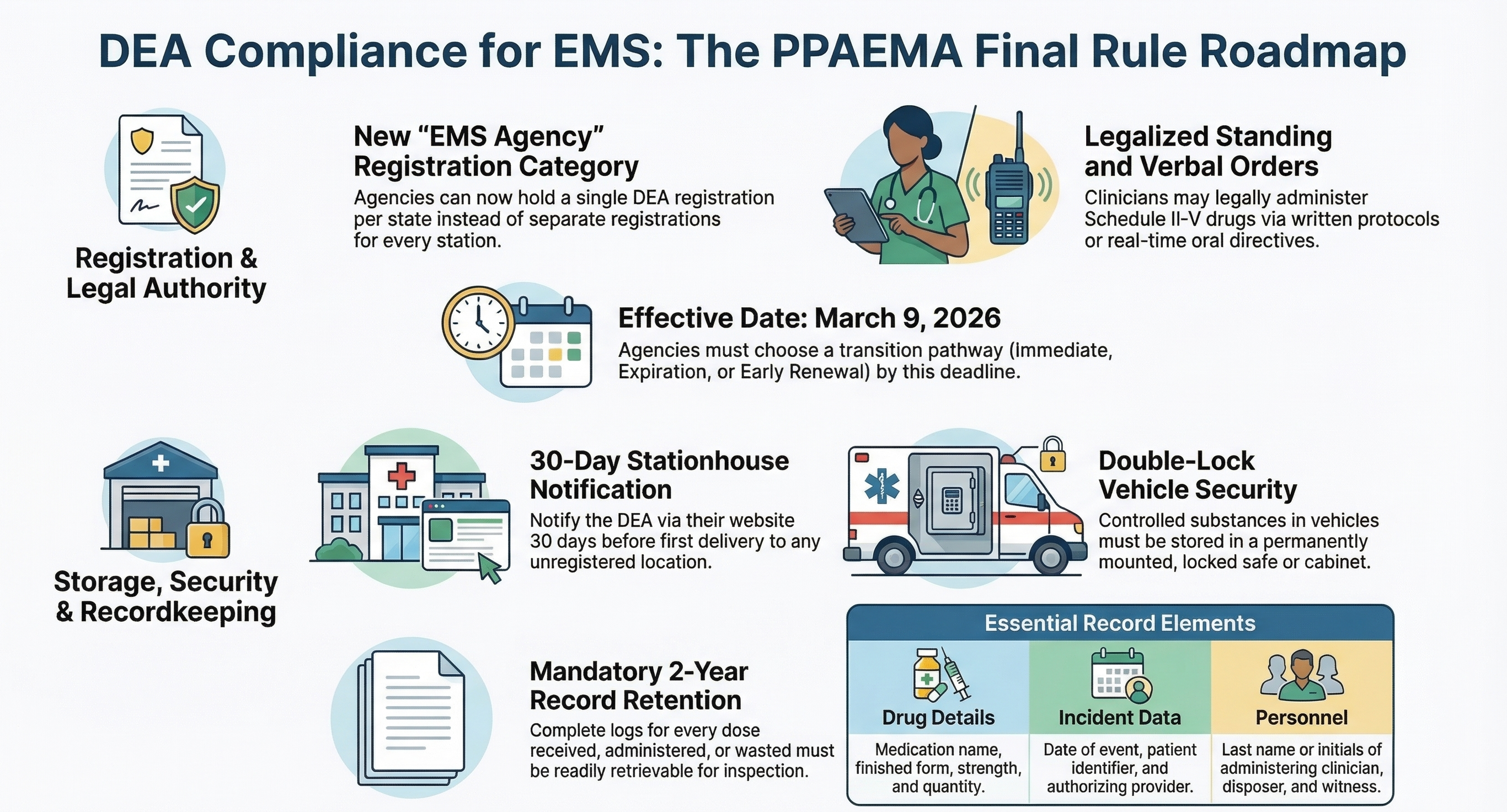
In 2017, the Protecting Patient Access to Emergency Medications Act (PPAEMA) was signed into law, and the Drug Enforcement Administration's (DEA) final rule implementing it officially took effect on March 9, 2026. This rule formalized the process for EMS agencies to hold their own DEA registrations, authorizing them to acquire, store, and administer Schedule II–V controlled substances in the field.
That registration comes with obligations — obligations that are becoming harder to meet with paper-based workflows. The DEA expects registrants to maintain accurate, continuous records of every controlled substance from the moment it enters an agency's possession until it is administered, wasted, or returned to a reverse distributor. In practice, this means documenting the chain of custody at every handoff point: pharmacy to registered location, registered location to designated stationhouse, stationhouse to unit, unit to provider, and back again.
What Counts as Adequate Documentation?
Adequate documentation, in the DEA's view, goes beyond a count on a clipboard. Agencies must ensure that their records are "readily retrievable" and maintained for a minimum of two years. To pass an audit, agencies should be prepared to demonstrate:
- A verifiable chain of custody for every controlled substance unit.
- Detailed, timestamped records of administration, waste, and returns. Under the new rule, there are 11 specific elements required for each dose administered or disposed of, including the drug name, date, patient identifier, amount given, the last name or initials of the administering professional, and the last name or initials of the medical director who issued the standing or verbal order.
- Proper documentation of waste, including the manner of disposal and the last name or initials of both the disposer and a witness.
- Reconciliation between expected and actual inventory at each custody transfer, including initial and biennial inventories.
- Rapid retrieval of records during inspections or audits.
Paper-based logs can technically satisfy these requirements, but they create gaps that are difficult to defend during an audit — illegible handwriting, missing signatures, or counts that don't reconcile because a sheet was lost or filled out hours after the fact.
The Shift Toward Digital Accountability
Regulatory expectations are trending toward digital, real-time accountability. While the DEA has not mandated electronic tracking for EMS, the standard of what constitutes "adequate" recordkeeping is rising, and the final rule explicitly permits the use of electronic recordkeeping systems. Agencies that rely on paper logs face increasing scrutiny, especially when variances surface.
NarcTrack was built to meet this higher bar by default. Every custody movement is timestamped, every count reconciliation is logged, and the entire audit trail is instantly retrievable — no binders, no scanning, no guesswork. With mobile scanning, role-based permissions, and automated audit trails, NarcTrack achieves this level of compliance with minimal disruption to existing crew workflows.
Common Compliance Gaps in EMS
Even well-run agencies often discover compliance gaps when they audit their own processes. Some of the most frequent violations cited by DEA experts include:
- Spotty Recordkeeping: Relying on memory for end-of-shift counts, failing to conduct the required biennial inventory, or failing to retain DEA Form 222 purchase orders for the mandated two years.
- Improper Waste Documentation: Waste events documented without a verifiable witness signature, or using informal disposal methods (like flushing medications), which are strictly prohibited.
- Unsecured Vehicles and Bags: Leaving EMS vehicles unattended without locking them and securing medications in a substantially constructed, non-readily removable cabinet or safe. While crews can carry "jump bags" on their person during active emergency responses, medications must be returned to secure storage immediately afterward.
- Failure to Report Losses Promptly: Delays in reporting significant losses or thefts. By law, thefts must be reported to the local DEA field office in writing within one business day, followed by an electronic DEA Form 106.
- Lack of a Dedicated Point Person: Many agencies fail to designate a specific employee who understands the records inside and out and can act as the primary contact during a DEA audit.
These gaps don't necessarily indicate wrongdoing — but they make it impossible to prove nothing went wrong. That inability to provide proof is the core risk.
Preparing Your Agency
The agencies that will be best positioned as DEA oversight continues to evolve under the PPAEMA are those investing in documentation infrastructure now. That means moving from paper-based tracking to a system that provides:
- Automated chain of custody with digital signatures and role-based permissions.
- Real-time inventory visibility across units, stationhouses, and designated locations.
- Exception-based alerting when counts don't reconcile.
- Exportable audit packages for inspections and internal reviews.
NarcTrack was built specifically for this transition. It doesn't change how your crews work — it captures what they're already doing and turns it into a verifiable, audit-ready record that satisfies federal law.
Ready to see NarcTrack in action?
Talk to our team about how NarcTrack can help your agency build audit-ready medication accountability.