How to Detect and Prevent Medication Diversion in EMS
Diversion Is a Documentation Problem First
Most EMS leaders understand that medication diversion — the theft or misuse of controlled substances — is a serious issue with legal, clinical, and organizational consequences. In almost all instances, when controlled substances are stolen from an ambulance service, they are taken by a trusted employee who leverages their access to exploit the system. What's less well understood is that diversion almost always succeeds because of gaps in documentation, not because of gaps in supervision.
When a provider diverts medication, they exploit the same weakness every time: the inability of paper-based systems to correlate patterns across shifts, units, and personnel in real time. A single missing vial looks like a counting error. Two missing vials over two weeks still looks like a counting error. By the time the pattern becomes visible, it's been going on for months. Because the DEA's enforcement strategy increasingly focuses on data-driven analysis and risk indicators rather than isolated events, relying on manual logs leaves agencies vulnerable to systemic compliance failures.
Why Traditional Detection Methods Fall Short
Most agencies discover diversion through one of three channels:
- A co-worker reports suspicious behavior. Federal regulations actually require employees who have knowledge of drug diversion by a fellow employee to report it, and employers must treat these reports confidentially while they investigate.
- A patient reports inadequate pain management.
- An audit reveals irreconcilable count variances.
All three are reactive. By the time any of these triggers fire, the diversion has been ongoing, the agency's liability has accumulated, and the investigation will be expensive and disruptive. The consequences are severe: the diverter faces criminal liability and termination, while the agency and its medical director could face DEA monetary penalties, administrative sanctions, and even the suspension of their registration.
The fundamental problem is that paper logs — and even basic spreadsheet tracking — don't surface anomalies. They record events in isolation. Connecting those events to identify behavioral patterns requires digital systems purpose-built for the task.
What Early Detection Actually Looks Like
An effective diversion detection system doesn't wait for a complaint or an audit. It watches for patterns continuously:
- A provider whose patients consistently receive lower doses than protocol suggests, or who consistently wastes significantly larger amounts of high-value drugs (like fentanyl or morphine) compared to their peers.
- Count variances that cluster around the same person, unit, or shift.
- Waste events that occur without proper witness verification.
- Timing anomalies — medications signed out long before or after the documented call time, or discrepancies between the medication log and the electronic Patient Care Record (ePCR) indicating a drug was taken but not administered to the patient.
- Physical evidence of tampering, such as vials with glue on the caps, minute pinholes, or medications replaced with saline or water so the containers appear full.
No single one of these signals confirms diversion. But when a system can correlate them across time and personnel, it surfaces risk early enough for supervisors to investigate proactively — before the situation escalates.
Building a Prevention-First Culture
Detection technology is only half the equation. Agencies also need workflows and policies that reduce opportunity and create accountability:
- Require point-of-transfer counts — not end-of-shift reconciliation from memory.
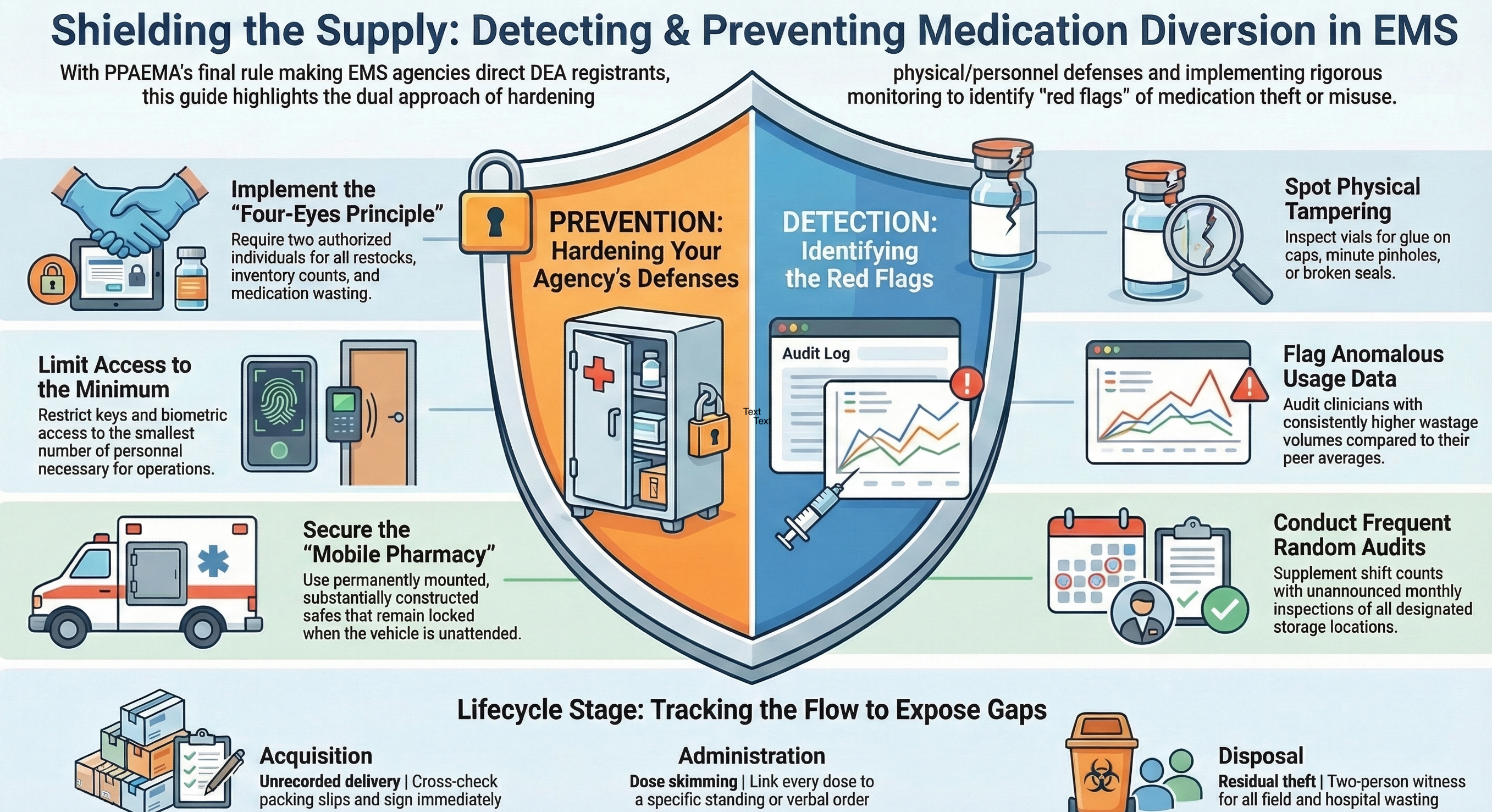
- Use digital signatures and witnessed verification for all waste events. The "four-eyes principle" dictates that no single individual should have unrestricted access to restocking cabinets, and all wastage should be witnessed and documented.
- Make custody logs accessible to supervisors in real time, not after-the-fact review.
- Conduct regular, randomized inventory audits — and ensure crews know they happen. Frequent audits are crucial; agencies conducting only quarterly or annual audits often miss substantial diversion until it's too late.
- Implement supportive measures, such as checking in with employees who are under severe stress or who have recently stopped taking prescribed pain medication, as they are statistically more likely to engage in diversion.
The goal isn't to create a surveillance culture. It's to build a system where the documentation is so routine and reliable that it protects honest providers as much as it deters bad actors.
How NarcTrack Supports Early Detection
NarcTrack's Diversion Risk Engine was designed around these principles. It monitors medication activity continuously and uses pattern analysis to flag potential concerns before they become confirmed incidents.
Rather than generating false alarms from isolated events, the engine evaluates behavioral trends across shifts, providers, and medication types. This aligns with modern DEA enforcement priorities, which emphasize a targeted, risk-based approach to identify patterns of diversion early. When thresholds are met, it creates a structured investigation workflow — complete with the relevant custody logs, count histories, and event timelines needed for supervisor review.
The result is faster detection, cleaner investigations, and a documented process that protects the agency and its personnel at every step.
Ready to see NarcTrack in action?
Talk to our team about how NarcTrack can help your agency build audit-ready medication accountability.